Hello, I’m Cynthia. I am 59 years old. I’ve always battled cravings for sweets—especially chocolate, which was a constant in my life. From childhood, staples of my diet consisted mainly of pasta, peanut butter, and potato chips. Every so often, I’d try to eat healthier by cutting back on fat, giving up chips, and adding more fruits and vegetables to my meals.
Ten years ago, in 2016, after watching documentaries on Netflix, I decided to prioritize my health. The movie that most inspired this change was entitled Fat, Sick & Nearly Dead. This documentary tells an emotional story of two men breaking their addiction to processed foods through a 60-day juice fast. The idea of the fresh fruits and vegetable fast is to reset your system. That helps you lose weight and reverse diseases.
Healthy Diet Failed
Following that advice led me to a disastrous year of veganism. I was confident that plant foods were good for me, so I ate my favorites—peanut butter and dark chocolate—daily. The results were nothing like what was promised. Rather than improving, my health declined into brain fog, pain, skin problems, constant hunger, and difficulty losing weight. Misery had set in, to stay.
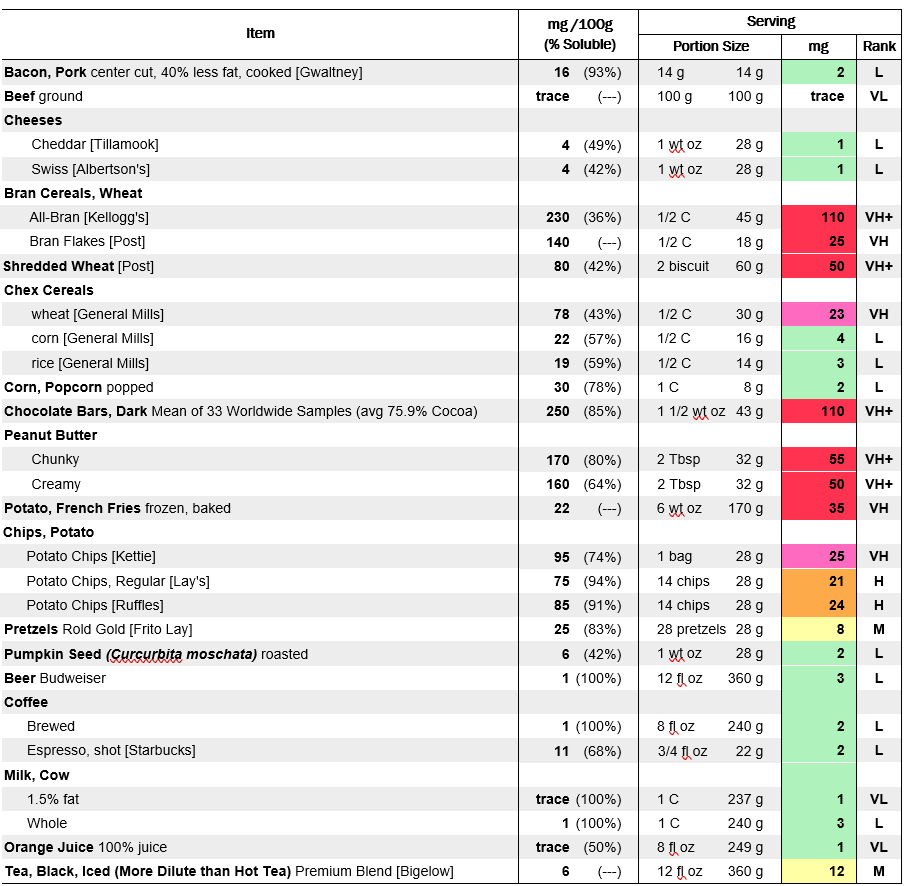
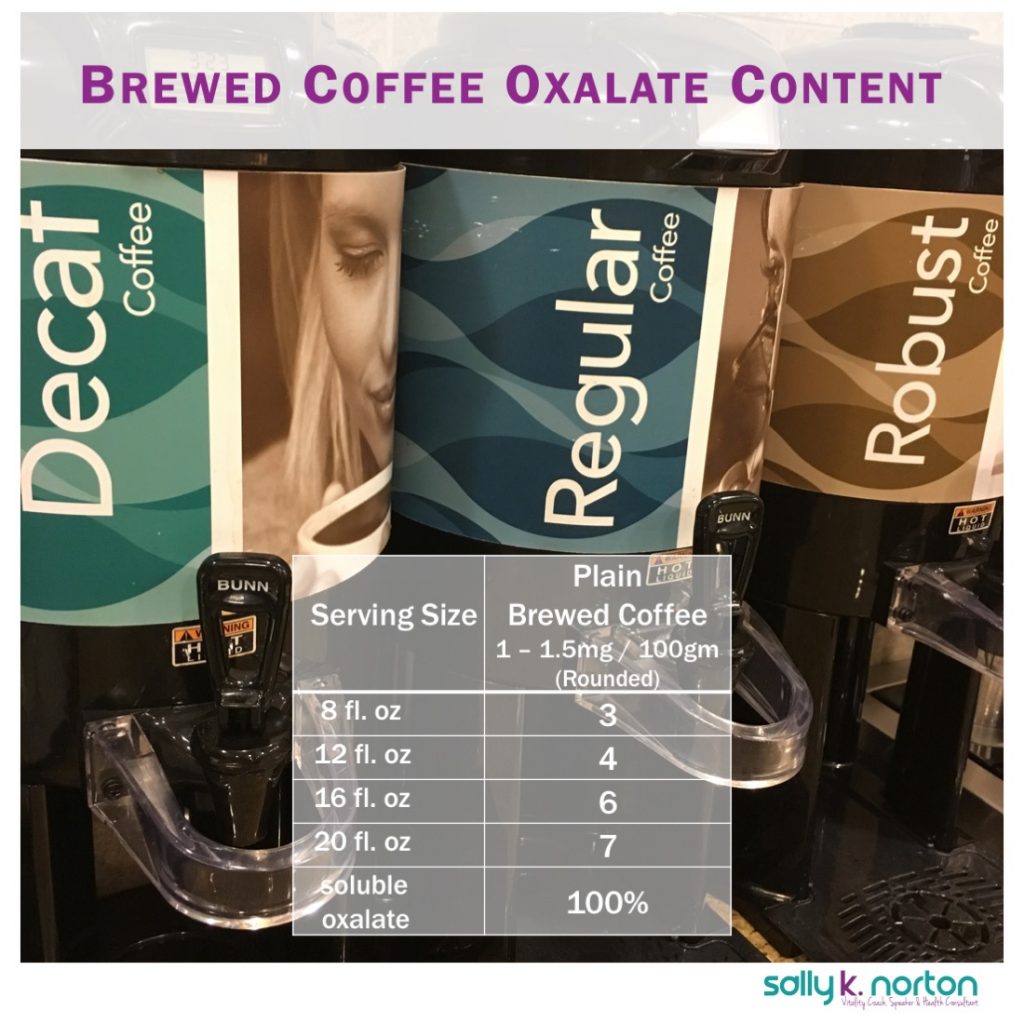
The solution was a shift to a low-carb, keto-style Paleo diet. Initially, I lost some weight and felt better, but something was still very wrong. I could never get into ketosis. I was eating mountains of almonds and almond flour, 85% dark chocolate, chia seeds, sweet potatoes, and huge bags of sautéed spinach that, when cooked, shrank to nothing. Discipline kept me on this keto diet, for years!
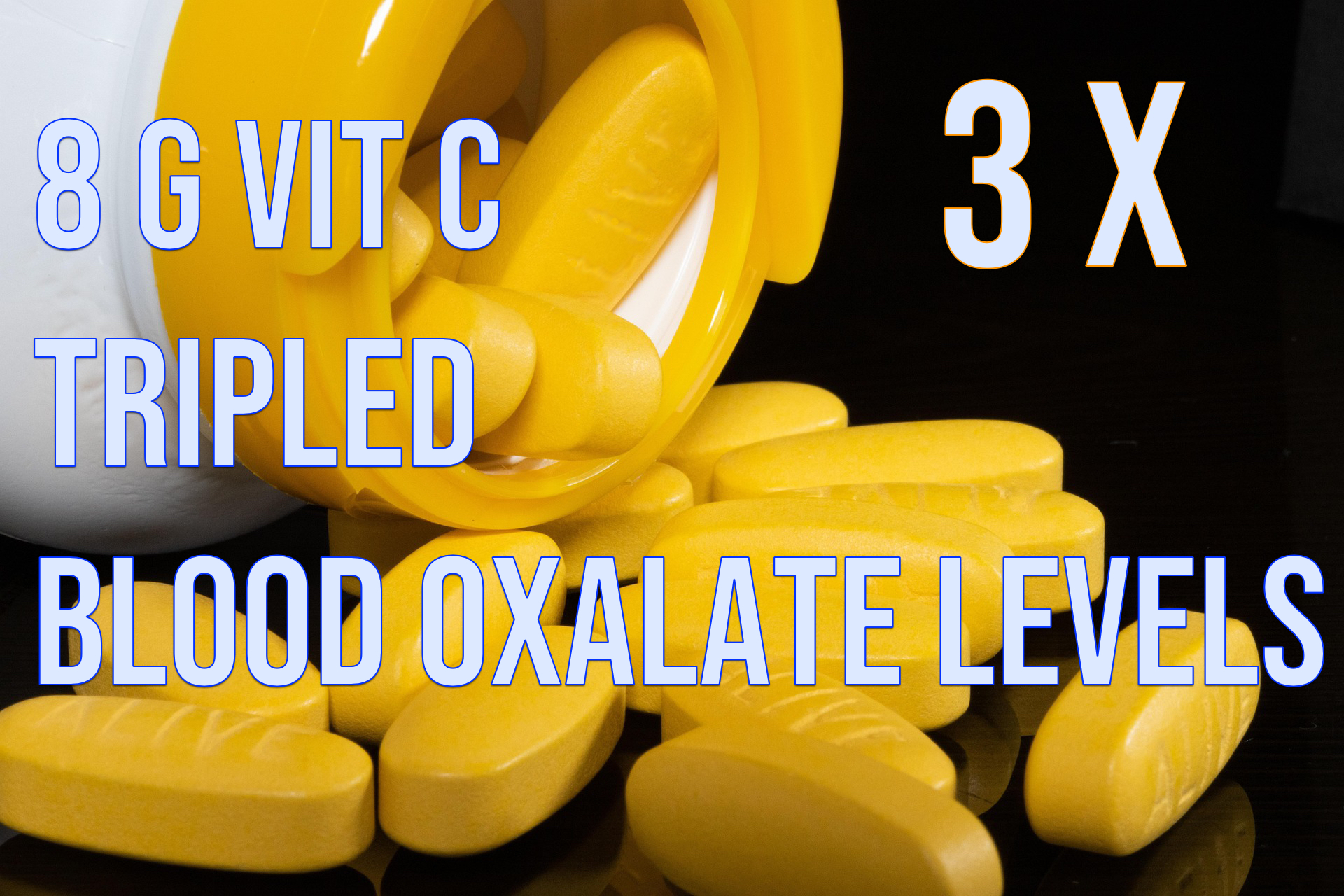
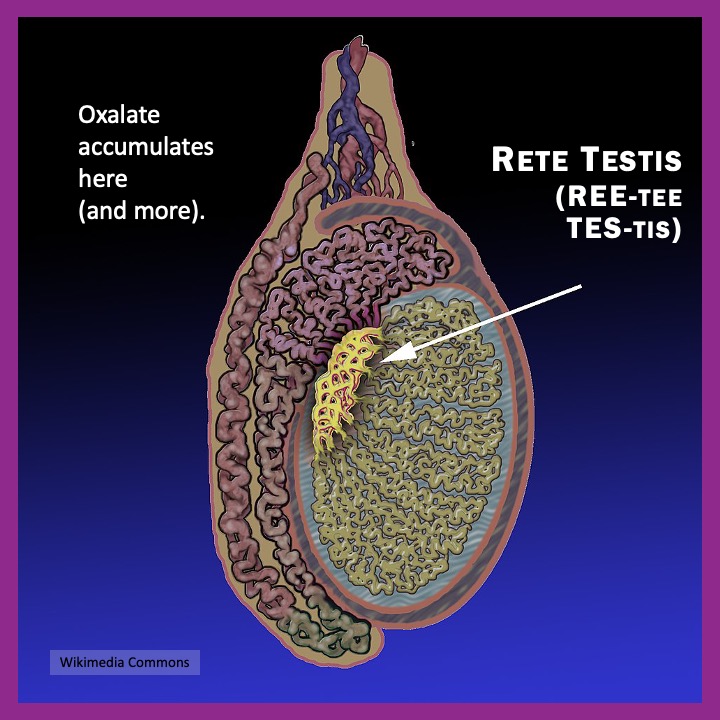
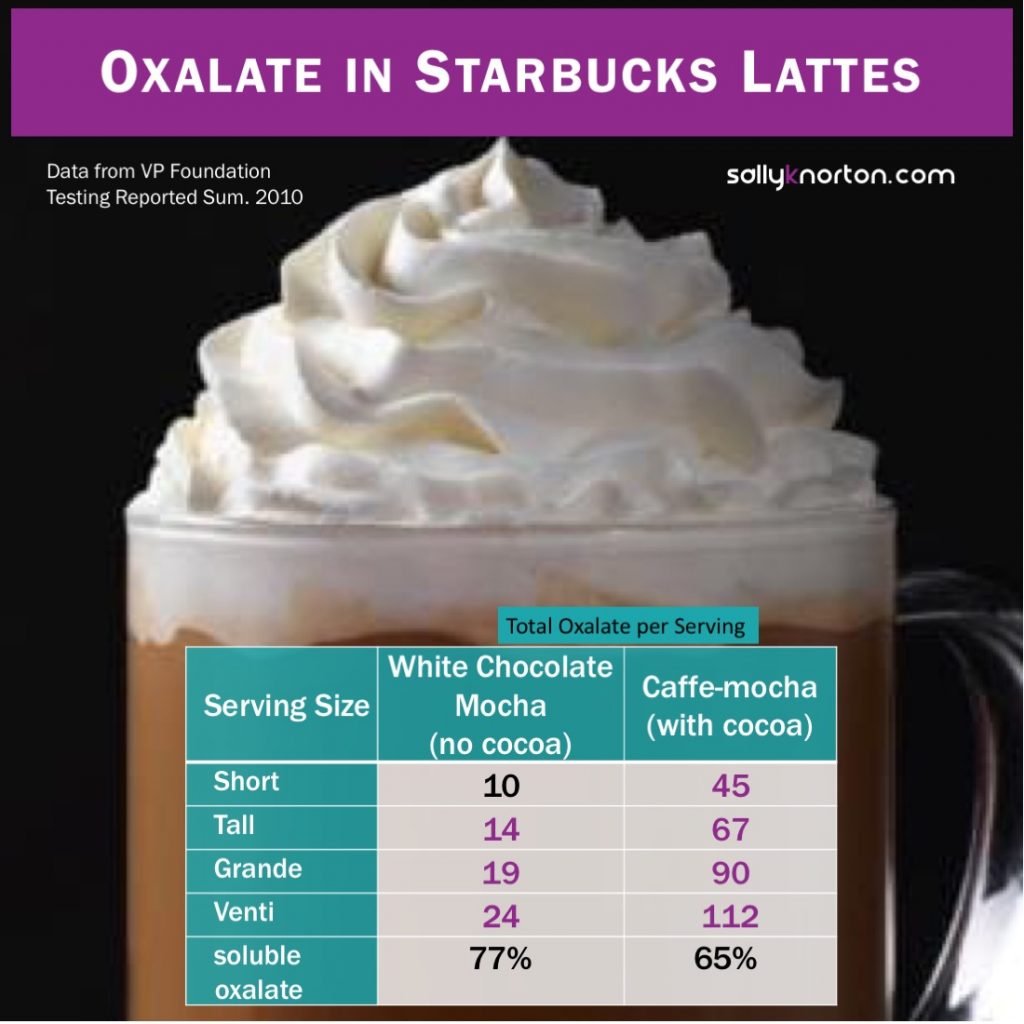
That created a massive oxalate overdose.

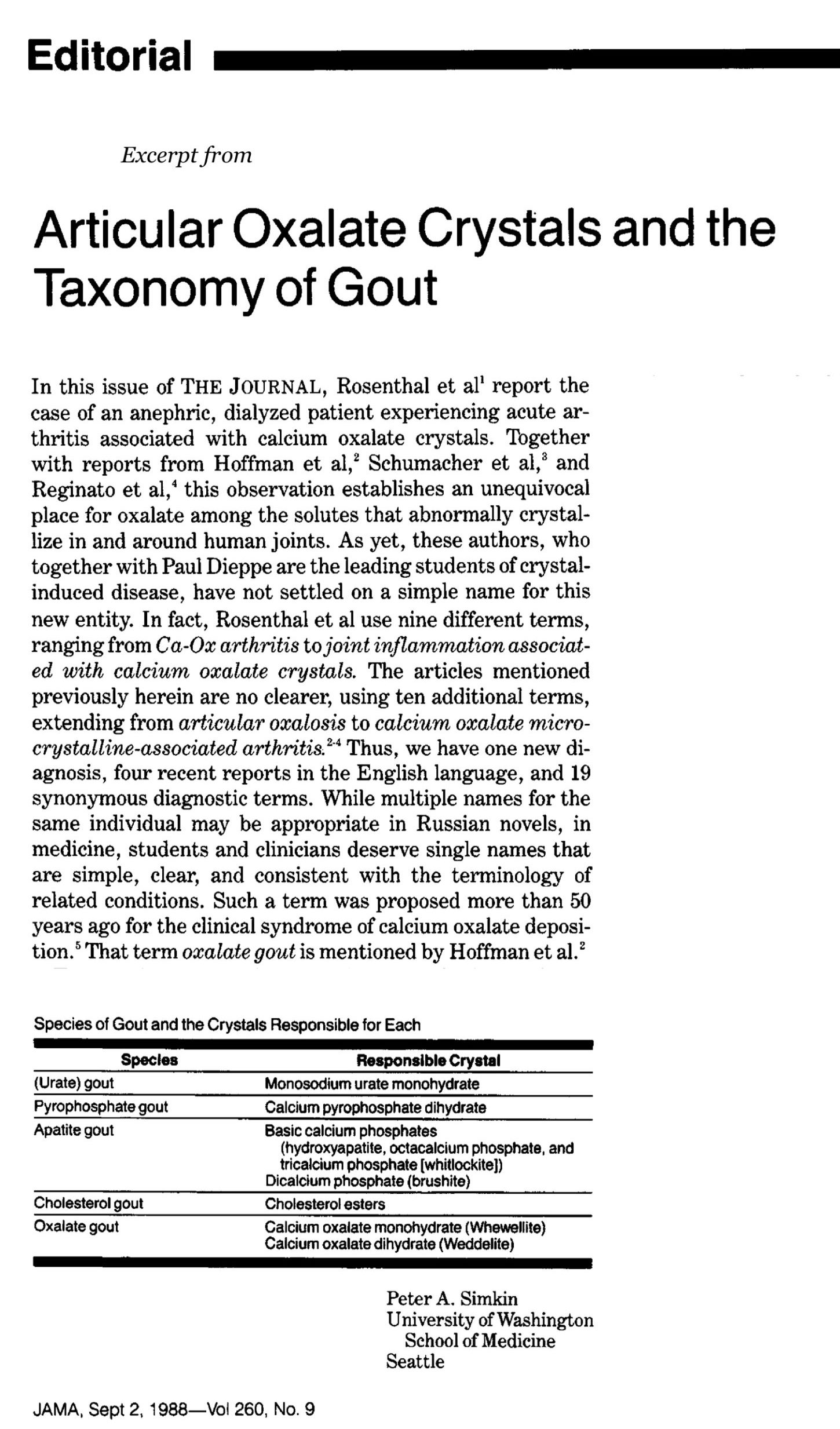
I was plagued with persistent health issues like fatigue, memory problems, pain, and anxiety. Switching to an all-meat carnivore diet in 2022 caused even more symptoms, which I later learned were caused by oxalate dumping triggered by removing all those high-oxalate foods.
I’m still deep in the clearing process, and it isn’t easy. But at least now I understand why. I’m finding my way back to my life and starting to have good days again—evidenced by my return to pickleball.
Cynthia is Back to Pickleball.


Lessons Learned
Looking back, I realize that my previous diet significantly harmed my health and career. Now, I know that no “superfood,” including chocolate, is worth the price: sacrificing my overall well-being.
I was misled about “healthy” eating, and as a result, I’m disillusioned with the medical field that I devoted my life to as a nurse. This experience showed me that many patients suffer from diet-driven issues that remain largely ignored in a system that rarely treats food as a root cause.