
Do you have painful gout, arthritis, bursitis, or stiff and swollen joints?

Pain is too Popular
Together, painful arthritis, gout, lupus, or fibromyalgia afflict over 53 million adults in the United States. As of 2014, twenty-seven percent of U.S. adults have chronic joint symptoms.[1] An earlier 2006 study revealed that even young people—over 8% of patients under the age of 20—complain of pain, typically in the feet, knees, or back.[2] Joint pain—arthritis and rheumatism—is the most common cause of disability in the U.S., affecting 9.1 million adults in 2010[3].
Chronic pain of one kind or another has become an expensive public health problem in the U.S., costing $635 billion in medical treatments and lost productivity in 2011 alone.[4] In 2016, Americans spent over $4 billion on pain-killing drugs that did nothing to address the cause of the pain[5]. And monetary cost estimates alone cannot begin to capture the losses associated with pain.
What if we could cheaply get out of pain? What if gout, arthritis, rheumatism, and back pain are a product of our diets—something very much under our individual control. Let’s take a closer look at gout.
What is Gout?
Gout is a form of inflammatory arthritis that can affect anyone. Sufferers experience sudden, severe attacks of pain, swelling, redness, and extreme tenderness in one or more joints, often the big toe, ankle, or fingers. The pain can have a burning quality as if the joints are on fire. Even after the acute gout pain subsides, joint discomfort may linger for days or weeks. With time, repeated attacks tend to last longer and affect more joints.
Gout and Diet
If you have gout, your doctor may be blaming your diet, and in particular the protein and salt you eat. The advice you’re likely to get? “Eat less meat and more low-fat vegetables.” Chances are such advice is tragically wrong.
Oxalate gout, a crystal-induced arthritis, as well as bursitis and tendinitis, can be caused by an oxalate-overloaded diet. Meats, fats, and salt don’t have oxalate, but dark chocolate, spinach, chard, almonds, buckwheat, peanuts, potatoes, and sweet potatoes do. Routine use of high oxalate foods can be the culprit in gout. When I had gout in college, I was a low-salt vegetarian. Thirty-some years later, I discovered that my gout was oxalate gout, caused by my vegetable-heavy diet, overloaded with oxalate.
Oxalate gout can appear, as it did for me, as a symptom of oxalate overload from my high-oxalate diet. But gout episodes can also occur during oxalate clearing as a transient symptom against the backdrop of improved health overall.
Crystals, Inflammation and Gout
Oxalate crystals forming and collecting in joints are known to trigger gouty inflammation and pain. The inflammation can be destructive to joint tissues. The accumulation of calcium crystals in cartilage (a.k.a. “calcification”) affects the elastic qualities of joints as well as their strength and stability. A lack of joint stability can cause pain. When I cut back on oxalate foods at age 49, my arthritis and long-standing foot problems (arising from weak connective tissues) finally disappeared.
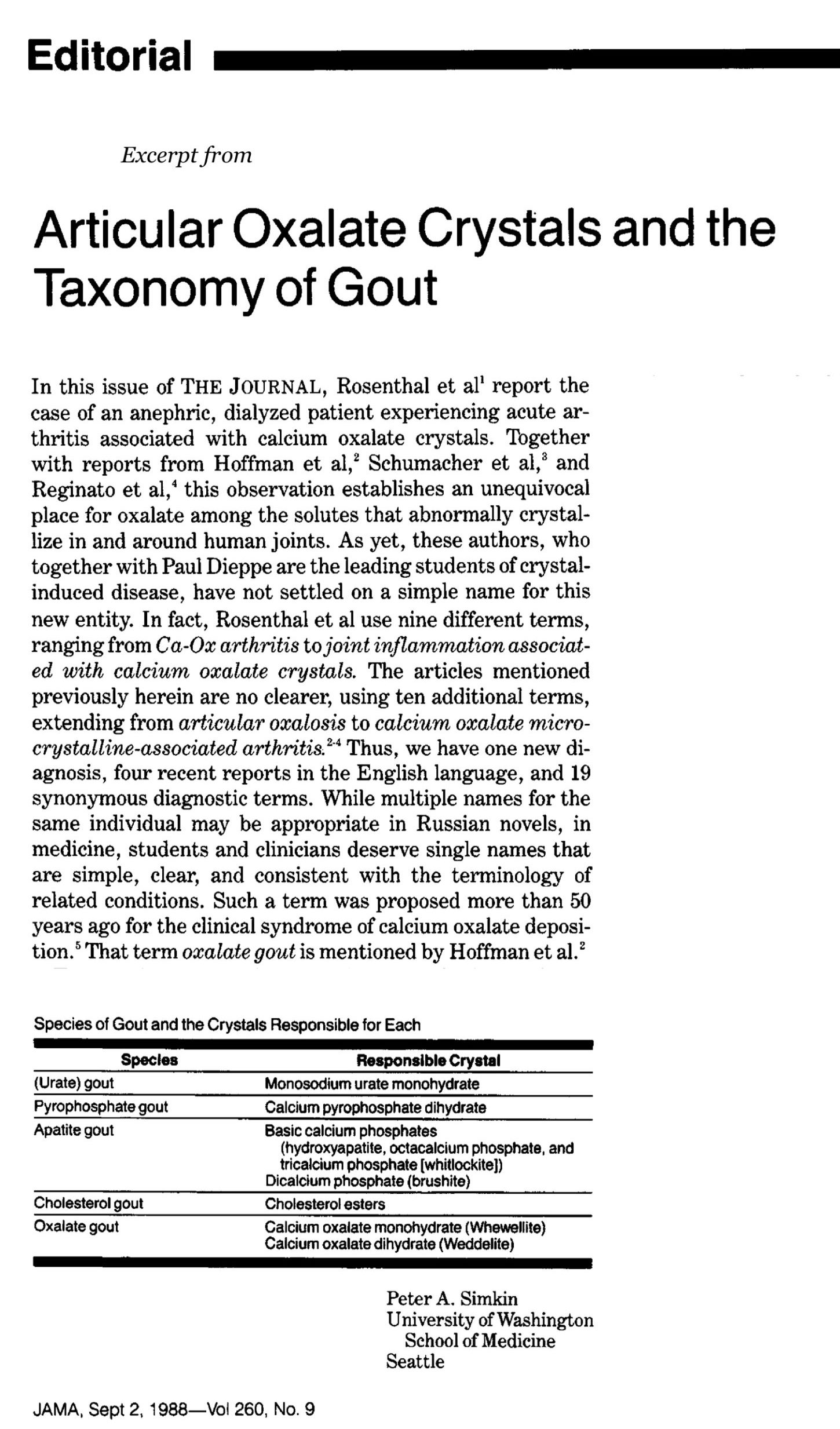
Being a toxic irritant, crystals within joints lead to acute or chronic inflammation including gouty arthritis. Oxalate is one of several crystal types associated with arthritis. In 1988, Rheumatologist and editor of the Journal of the American Medical Association (JAMA) Dr. Peter Simkin, pointed out that the medical field uses too many difficult terms including “articular oxalosis” and “calcium oxalate micro-crystalline-associated arthritis” when referring to oxalate gout. The lack of simple, clear, and consistent terms for the various types of gout, especially oxalate gout, interferes with the clinical recognition of oxalate gout.
Oxalate is Hard to See
Diagnosis distinguishing one type of gout from another is problematic and depends on elusive analysis of joint fluid. Several authors, including rheumatologist and medical textbook author Antonio Reginato, call out the difficulty of identifying calcium oxalate crystals in synovial fluid of joints because they can easily be confused with other crystals.[6] Reginato’s work helped to establish the connection between crystals in joint spaces and arthritis and other bone and joint symptoms.
Invisible oxalate nanocrystals and oxalate ions are reactive and mobile, and thus are more toxic than the “prominent” crystals that are typically discovered by pathologists.[7] Slow to notice even the visible crystals, researchers, doctors, and pathologists are even slower to imagine the possibility of toxic trace deposits of nanocrystals and other chemical forms of oxalate in tissues. Although we can’t see them, nanocrystals do the most damage because of their ability to enter cells. And collectively, they have a larger surface area that interacts with living tissues.[8] Consequently, they are simultaneously stealthy, undetectable, and harmful.
Oxalates can also collect in tissues in other difficult to detect forms. In 1967, researchers Zarembski & Hodgkinson noted the presence of a non-crystalline complex of calcium and lipid in the liver and intestine: the oxalate lipids. [9] Similarly Reginato reported findings of lipid crystals and inflammation in joint fluids from patients with gout, rheumatoid arthritis, and traumatic bursitis.[10] He explains that analysis of joint fluids is rarely performed in cases of oxalosis, although joint pain is a known problem for these patients.
Another experiment led by a Belgian hematologist exposed human serum and dishes of living human cells that line blood and lymphatic vessels to oxalate crystals. They confirmed that oxalate crystals collect in blood vessel walls and trigger the immune cell reactions associated with the pain of gout and vasculitis[11].
Accepted clinical standards seem to miss the connection between oxalate and joint pain. Gout is strongly associated with kidney stones and chronic kidney disease. Despite this association, gout patients are typically excluded from studies on oxalate kidney stones. That is unfortunate given that high levels of oxalate (promoting stones anywhere in the body) seem to encourage uric acid gout and oxalate gout.
the formation and accumulation of crystals in tissues is a hallmark of many metabolic and inflammatory conditions, not just kidney and bladder problems.
Other Reasons High Oxalates Create Pain
Based on existing science, let me explain why minimizing oxalate exposure can get at the root cause of inflammatory problems and solve chronic pain problems. Science now recognizes that crystals forming in tissues are part of the development of gout and atherosclerosis[12]. Many studies have demonstrated that calcium oxalate crystals cause renal inflammation and damage renal immune cells[13]. In fact, the formation and accumulation of crystals in tissues is a hallmark of many metabolic and inflammatory conditions, not just kidney and bladder problems.
In addition to oxalate collecting in joint spaces, tendons, cartilage, and bones, oxalate causes nerve damage that creates pain, and increases uric acid, which is also associated with joint pain and gout. Most doctors blame uric acid for gout symptoms, which is elevated in people with oxalate kidney stones.
Inflammation
When oxalic acid grabs calcium and changes into crystals, calcium oxalate nanoparticles activate human monocyte cells and enhance local tissue inflammation[14]. That process and the related cell damage stirs up defensive innate immune system actions. These actions include “foreign body” alerts and “inflammasome” reactions, which call in platelets, causing tissue damage and promoting the development of auto-immune symptoms and fibrosis.
The immune engagement caused by exposure to high levels of either oxalate ions or oxalate crystals can lead to inflammatory conditions such as intermittent and chronic pain[15]. Oxalic acid ions and crystals create free radicals in cells that stimulate immune cells to secrete an immune signaling protein called MCP-1 (Monocyte chemoattractant protein-1). MCP-1 is implicated in the development of many diseases, including cancers, neuroinflammatory diseases, rheumatoid arthritis, and cardiovascular disease.
Aside from mechanical damage to the tissues, oxalate can also have a dramatic effect on cell physiology, including inhibiting the immune response to infection and shifting immune system toward uncontrolled inflammation.
Long before oxalates become crystals in tissues, oxalic acid damages immune cells (macrophages) and puts them in a pro-inflammatory state (with reduced cellular energy, increased oxidative stress, and damaged mitochondria)[16]. Dr. T. Mitchell’s team at the University of Alabama found damage to circulating immune cells in their human volunteers just 40 minutes after giving them a spinach smoothie with 720mg of oxalate[17].
Famous Gout Sufferers
Queen Anne (b. 1665, d. 1714)

The famously gouty monarch of Great Britain and Ireland, Queen Anne, experienced bouts of pain in her limbs, stomach, and head. Today’s doctors may have said she had systemic lupus and pelvic inflammatory disease.
Anne Stuart suffered from other illnesses too—diseases associated with modern foods like tea, chocolate, and way too much refined carbohydrate: diabetes, nutrient deficiency, and probably oxalate overload.
Not only was she morbidly obese and diabetic at age 30, but pain also tormented her. By age 33, Queen Anne’s gout was a migratory arthritis affecting many of her joints, especially her feet, knees, and hands. The debilitating joint pain prevented walking: in 1702 she was carried to her coronation in a sedan chair. She was 35. She also had other forms of chronic inflammation: headaches, stomach pain, skin problems (red and spotted face eruptions that coincided with her bouts of joint pain).
Her issues suggest that her high oxalate diet was likely a factor behind her suffering.
In childhood, sickly Anne was sent to France for treatment of a serious eye condition with excessive discharge known as “defluxion.”[18] (Some of my clients report copious fluid draining from their eyes with fine grit in it.) While she lived with her French relations as a child, she was introduced to using chocolate, sweets, and tea to help her cope. Anne loved all things sweet.
She adopted a habit of a nightly cup of sweetened hot chocolate. Anne also enjoyed tea every day. Even more so than chocolate, tea was a great exotic novelty of her age, initially popular with the Dutch and French (she had Dutch family and married a Dutchman).
Irish Anglian cleric and author of Gulliver’s Travels, Jonathan Swift (1667 – 1745) was a contemporary of Queen Anne. Swift, who frequented taverns serving hot chocolate, or “chocolate houses,” wisely blamed gout on the over-consumption of chocolate. (According to Wikipedia, Swift hoped for a church appointment in England, but the Queen disliked Swift, finding his first book, A Tale of a Tub (1704), blasphemous.)
The severity of Queen Anne’s symptoms was both cyclical and progressively worsening until her death in 1714 at age 49. Some scholars speculate that the ultimate cause of death was kidney failure.
Ben Franklin
Decades later, in 1780, American founding father Ben Franklin was bedridden with gout. Pen in hand, he asked, “What have I done merit to these cruel sufferings?” ‘Madam Gout’ had an answer. She told him his gout was due, in addition to his sedentary amusements, to his “inordinate breakfast, four dishes of tea with cream, and one or two buttered toasts . . .” People had been drinking tea from china bowls (without handles) since Queen Anne’s day. When she ruled England, tea had been around for just a few decades; by Franklin’s time, tea was standard daily fare in Great Britain and its territories.
Science Explains the Connection Between Tea, Chocolate and Pain
In the early 1940’s, researchers produced dramatically stunted growth in rats by adding 16% cocoa to their normal diet. They concluded that “indiscriminate and excessive use of chocolate flavored foods, especially in a diet already low in calcium, is not to be recommended”[19]. Today it’s easy to consume a diet consisting of 16% high oxalate foods like chocolate (and lots of sugar too). Yet, chocolate is now heralded as a health food. Previous generations knew better: two of our long-favored stimulants, chocolate and tea were not to be trusted.
Healing story of Joint Pain Relief with Diet
I have heard and have witnessed many remarkable cases of relief from joint pain after the removal of high oxalate foods from our diets.
My husband who developed debilitating carpal tune syndrome in the wake of the high-oxalate diet he adopted after we met reversed it with a low-oxalate diet.
My friend Ron mentioned in Chapter 13 of Toxic Superfoods also reversed pain in his thumb joints.
Many others have shared their stories online or written me directly, as did this woman from Australia. She is over-joyed to have relief from 8-years of gout. Here is her story:
Dear Sally,
I came across your work through Dr. Bill Schindler who was being interviewed on Episode 108 of the WildFed Podcast. My ears perked up as he was describing his health issues with gout and he explained how he had discovered your work with oxalates. My eyes widened and jaw dropped! I have been suffering from gout for the last 8 years. My mind was completely blown! I felt like a 1000-piece puzzle just fell completely into place at once.
Chard (silverbeet greens), tahini, dark chocolate, almonds, and sweet potatoes were all a part of my “healthy” diet. I expected they would get my gout pain to subside.
I have now been on a low-oxalate diet for three months and my gout has entirely disappeared. My receding, brittle fingernails are looking the best that they ever have and the eczema around my mouth (which I have always had and thought was a dairy related issue) is completely gone.
Since hearing that interview, I have immersed myself in your work. I’ve read and listened to everything that I can find!
From the bottom of my heart, thank you so much for the work that you are doing. The gratitude that I feel is beyond words. Thank you for your passion, your love, your genuine care for people, and your integrity. You are changing lives!
Reversing Oxalate Crystal Deposits in Joints: It’s not over until it’s over
Though low-oxalate eating can lead to remarkable improvement from gout and other joint and connective tissue conditions, gout can also be a symptom of oxalate clearing. When recovering from oxalate overload and enjoying overall improvements in health, the immune system’s efforts to remove oxalate from joint tissues can provoke occasional gout attacks in some people as they recover. The process can take years, but these painful episodes become less frequent and eventually end, seemingly for good.
Footnotes
[1] CDC, “Age-Adjusted Percentages of Selected Diseases and Conditions Among Adults Ages 18 and over, by Selected Characteristics: United States, 2014 Summary Health Statistics: National Health Survey, 2014 Table A-4a” (U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics, 2014), http://ftp.cdc.gov/pub/Health_Statistics/NCHS/NHIS/SHS/2014_SHS_Table_A-4.pdf.
[2] Albert Tan et al., “Epidemiology of Pediatric Presentations with Musculoskeletal Problems in Primary Care,” BMC Musculoskeletal Disorders 19, no. 1 (06 2018): 40, https://doi.org/10.1186/s12891-018-1952-7.
[3] Theis, K. A., Steinweg, A., Helmick, C. G., Courtney-Long, E., Bolen, J. A., & Lee, R. (2019). Which one? What kind? How many? Types, causes, and prevalence of disability among U.S. adults. Disability and Health Journal, 12(3), 411–421. https://doi.org/10.1016/j.dhjo.2019.03.001
[4] Institute of Medicine (US) Committee on Advancing Pain Research.
[5] “OTC Sales by Category,” accessed December 12, 2017, https://www.chpa.org/OTCsCategory.aspx.
[6] A. J. Reginato and B. Kurnik, “Calcium Oxalate and Other Crystals Associated with Kidney Diseases and Arthritis,” Seminars in Arthritis and Rheumatism 18, no. 3 (February 1989): 198–224.
[7] Xin-Yuan Sun et al., “Mechanism of Cytotoxicity of Micron/Nano Calcium Oxalate Monohydrate and Dihydrate Crystals on Renal Epithelial Cells,” RSC Advances 5, no. 56 (May 18, 2015): 45393–406, https://doi.org/10.1039/C5RA02313K.
[8] Xin-Yuan Sun et al., “Size-Dependent Toxicity and Interactions of Calcium Oxalate Dihydrate Crystals on Vero Renal Epithelial Cells,” Journal of Materials Chemistry B 3, no. 9 (February 18, 2015): 1864–78, https://doi.org/10.1039/C4TB01626B.
[9] P. M. Zarembski and A. Hodgkinson, “Plasma Oxalic Acid and Calcium Levels in Oxalate Poisoning,” Journal of Clinical Pathology 20, no. 3 (May 1967): 283–85.
[10] Reginato, A.J., and Kurnik, B. (1989). Calcium oxalate and other crystals associated with kidney diseases and arthritis. Semin. Arthritis Rheum. 18, 198–224.
[11] M. A. Boogaerts et al., “Mechanisms of Vascular Damage in Gout and Oxalosis: Crystal Induced, Granulocyte Mediated, Endothelial Injury,” Thrombosis and Haemostasis 50, no. 2 (August 30, 1983): 576–80.
[12] Franklin, B.S., Mangan, M.S., and Latz, E. (2016). Crystal Formation in Inflammation. Annual Review of Immunology 34, 173–202. 10.1146/annurev-immunol-041015-055539.
[13] Mulay, S.R., Kulkarni, O.P., Rupanagudi, K.V., Migliorini, A., Darisipudi, M.N., Vilaysane, A., Muruve, D., Shi, Y., Munro, F., Liapis, H., et al. (2013). Calcium oxalate crystals induce renal inflammation by NLRP3-mediated IL-1β secretion. J Clin Invest 123, 236–246. 10.1172/JCI63679.
[14] Mulay, S.R., Herrmann, M., Bilyy, R., Gabibov, A., and Anders, H.-J. (2019). Editorial: Nano- and Microparticle-Induced Cell Death, Inflammation and Immune Responses. Front Immunol 10, 844. 10.3389/fimmu.2019.00844
[15] Umekawa, T., Chegini, N., and Khan, S.R. (2002). Oxalate ions and calcium oxalate crystals stimulate MCP-1 expression by renal epithelial cells. Kidney Int 61, 105–112. 10.1046/j.1523-1755.2002.00106.x.
[16] Kumar, et al 2021 Oxalate Alters Cellular Bioenergetics, Redox Homeostasis, Antibacterial Response, and Immune Response in Macrophages.
[17] Kumar, et al 2021. Dietary Oxalate Loading Impacts Monocyte Metabolism and Inflammatory Signaling in Humans.
[18] https://www.willowandthatch.com/history-queen-anne-britain-favourite/; https://www.historyofroyalwomen.com/anne-queen-of-great-britain/queen-anne-an-unhealthy-life-part-three/
[19] W. S. Mueller and M. R. Cooney, “The Effect of Cocoa upon the Utilization of the Calcium and Phosphorus of Milk.,” Journal of Dairy Science 26 (1943): 951–58, https://doi.org/0.3168/jds.S0022-0302(43)92791-2.
See Also:
Hoffman, G.S., Schumacher, H.R., Paul, H., Cherian, V., Reed, R., Ramsay, A.G., and Franck, W.A. (1982). Calcium oxalate microcrystalline-associated arthritis in end-stage renal disease. Ann. Intern. Med. 97, 36–42.





