Chocolate has been rebranded. A confectionery indulgence is now
- “rich in flavanols”
- “cardioprotective”
- longevity insurance, and
- a medical intervention.
We’re told dark chocolate lowers blood pressure, improves insulin sensitivity, enhances mood, protects the brain, and even supports heart health. The higher the cacao percentage, the more medicine-like dark chocolate becomes.
Health Halo Built on Inflated Science
Most of the glowing claims rely on studies using isolated cocoa flavanol extracts at doses far higher than those in commercial chocolate. To reach those levels through ordinary chocolate, a person would have to consume impractical—and metabolically costly—amounts. What real chocolate delivers is calories, sugar, fat, oxalate, and heavy metals. All are worthy of ignoring in favor of its mythical powers.
News headlines, social media posts, or wellness marketing will not whisper any caution or caveats. Its failure to deliver doesn’t trend, and won’t be found in captions, or even the fine print.
What the Metabolic Data Show
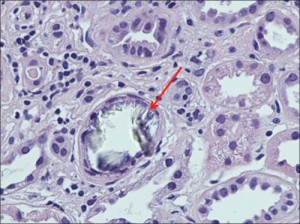
Chocolate is naturally high in oxalate. Oxalate is the compound central to calcium oxalate kidney stone formation. In 1989, researchers published in Nephron (Balcke et al.) demonstrated that consuming 50–100 grams of chocolate increased urinary oxalate excretion to 235–289% of fasting levels in healthy men.
These peak blood and urine values are comparable to those observed in primary hyperoxaluria, a deadly metabolic disorder known to cause vasculitis (inflammation that destroys blood vessels), bone loss, kidney failure, and early death.
Five years later, Nguyen et al. (1994) reported in Hormone and Metabolic Research that a single 100-gram dark chocolate bar increased urinary calcium by 147% and urinary oxalate by 213% within hours. That pairing—hypercalciuria plus hyperoxaluria—produces precisely the urinary chemistry known to favor calcium oxalate stone formation.
Unlike the familiar “flavanols are medicine” narrative, these findings were not speculative. They were controlled metabolic measurements.

Further nephrology research has clarified why this matters. Robertson and Peacock (1980) showed that urinary oxalate correlates more strongly with calcium oxalate stone formation than urinary calcium. Jaeger and Robertson (2004) detailed how dietary oxalate is absorbed throughout the gastrointestinal tract, depending on solubility, calcium availability, and intestinal conditions.
Subsequent studies by leading oxalate researchers demonstrated that dietary oxalate contributes substantially more to urinary oxalate than previously believed. Holmes et al. (2001) estimated that up to 50% of urinary oxalate may originate directly from dietary sources, particularly when dietary calcium is insufficient. Meals produce sharp spikes in urinary oxalate concentration, followed by wash-out periods during fasting—conditions that may favor intracellular crystal formation and tissue injury.
In practical terms, this means oxalate is not inert.
It is absorbed. It circulates. It is managed. It must be excreted. The process is stressful for cells and tissues. Repeated exposure means repeated spikes—and accumulation. That is inflicting damage you cannot see. None of this appears in glossy “eat more dark chocolate” features.
Heavy Metals: The Other Omission
Oxalate isn’t the only missing piece.
Food-safety literature on cocoa and chocolate (Winkler, 2014) focuses heavily on contamination control, because cocoa is vulnerable to heavy metals. Cadmium and lead contamination are well-documented issues in commercial chocolate products.
Heavy metals accumulate. They do not enhance vascular function. They do not reverse aging. They increase the toxic burden. The health halo message rarely includes that caveat.
A Halo Was Built on “Nutrifluff”
This silence about dose and toxins in chocolate is not accidental.
In 2018, Nic Fleming’s Guardian investigation, “The Dark Truth About Chocolate,” described how industry funding, selective framing, and careful messaging helped elevate chocolate from confectionery to cardiovascular ally. He wrote, “Many people have swallowed the idea that chocolate is a ‘superfood’. Except it isn’t.”
Many cocoa studies examined isolated flavanol extracts at pharmacologic doses. Initially, scientific observations were issued cautiously. But then wishfully and prematurely stretched into widely accepted lifestyle advice: “eat darker chocolate and more of it.”
Sensational research findings from highly preliminary studies about a single food or nutrient get flattened into headlines. “May improve endothelial function” became “good for your heart.” Nutrition scientist Marion Nestle has a word for this kind of phenomenon: “nutrifluff.” Real studies — selectively amplified — until they resemble proof.
The science didn’t have to be fraudulent, just short-sighted. It’s too easy to see what we want to see and ignore the rest.
Science Hoax Believed
Case in point how the system seems vulnerable to fantasy and exaggeration, remember the 2015 “Slim by Chocolate” hoax. Multiple journals accepted a deliberately fake and flawed “study” claiming that eating chocolate could aid weight loss, without thorough peer review. Despite the obvious flags—published in a journal with questionable credibility and a small sample size—the science media fell for it.
Major news outlets worldwide proclaimed, “Chocolate Can Help You Lose Weight!” Routinely, science journalists fail in their duty to rigorously fact-check or look for a more balanced attitude in their reporting. Being the first to report sizzle matters more than being factually correct and skeptical.
The Medical Endorsement of Weak Science
It’s worth noting that the chocolate health narrative didn’t emerge from nowhere.
“Industry-funded research tends to set up questions that will give them desirable results,” Fleming explains. “Chocolate manufacturers have poured huge sums into funding nutrition science that has been carefully framed, interpreted and selectively reported to cast their products in a positive light over the last 20 years.”
It may be especially easy for researcher to find positive outcomes for chocolate eating. Study volunteers, like most people, have positive expectations about chocolate because they like it. They are therefore primed, preconditioned – to respond positively. Pleasure just might lower blood pressure, for example.
Registered dietitians, cardiologists, and academic researchers have publicly commented on potential benefits of cocoa flavanols — particularly for blood vessel function, circulation, and blood pressure. Institutions such as Johns Hopkins Medicine and NIH-funded researchers have discussed observational findings, including studies of the Kuna people, whose traditional cocoa consumption sparked decades of scientific interest.
These expert reports are typically referring to flavanol compounds — not candy bars. Generally they emphasize caveats: high-cocoa content and context of moderation within an otherwise complete or varied diet, not daily therapeutic dosing.
A more complete story is inconvenient
The antioxidant narrative was seductive — and largely uncontested. Seeking only the good news, researchers never asked what comes with flavanols in real chocolate: oxalate load, mineral disruption, cadmium, and lead. Enthusiasm for positive publishable results and a media-friendly topic gained a life of its own. Adding nuance and a dose of reality would just spoil the party.
Once marketing took over, there was no room for the biological costs. Oxalates, heavy metals, mineral disruption—who cares? You need to care.
Spin or Informed Awareness?
Chocolate does not have to prove itself medicinal. The spin only has to sound plausible. The real risk is the belief built on the myth—strong enough to:
- fuel a marketplace built on false promises,
- shape thinking, daily habits, and shared culture,
- create blinders.
Willful ignorance does not build a healthy future. When a food that can raise urinary oxalate by nearly 300% is marketed as preventive medicine, that’s malpractice. Acknowledging this isn’t fearmongering. It’s informed awareness.
Chocolate is not cardiovascular therapy. It is candy with a marketing department.
Enjoy it occasionally, if you choose—but let’s retire the fiction that an 85% label turns chocolate into healthcare.
Respect your biology, and don’t confuse branding with medicine.

Selected References
Balcke, P., Zazgornik, J., Sunder-Plassmann, G., et al. (1989). Transient hyperoxaluria after ingestion of chocolate as a high-risk factor for calcium oxalate calculi. Nephron, 51(1), 32–34
Bohannon, J. (2015). I Fooled Millions Into Thinking Chocolate Helps Weight Loss. io9.
Fleming, N. (2018). The Dark Truth About Chocolate. The Guardian.
Henkel, R., & Agarwal, A. (2020). Harmful Effects of Antioxidant Therapy. In S. J. Parekattil, S. C. Esteves, & A. Agarwal (Eds.), Male Infertility: Contemporary Clinical Approaches, Andrology, ART and Antioxidants (pp. 845–854). Springer International Publishing. https://doi.org/10.1007/978-3-030-32300-4_68
Holmes, R. P., Goodman, H. O., & Assimos, D. G. (2001). Contribution of dietary oxalate to urinary oxalate excretion. Kidney International, 59(1), 270–276. https://doi.org/10.1046/j.1523-1755.2001.00488.x
Jaeger, P., & Robertson, W. G. (2004). Role of dietary intake and intestinal absorption of oxalate in calcium stone formation. Nephron Physiology, 98(2), 64–71.
Nguyen, N. U., Henriet, M. T., Dumoulin, G., et al. (1994). Increase in calcinuria and oxaluria after a single chocolate bar load. Hormone and Metabolic Research.
Robertson, W. G., & Peacock, M. (1980). The cause of idiopathic calcium stone disease: Hypercalciuria or hyperoxaluria? Nephron, 26(3), 105–110.